Hip Replacement Surgery Raleigh NC
Most of my patients go home the same day of surgery or by the next day. I believe the sooner you get home and leave the hospital setting, the lower the risk for a surgical wound infection.
Total hip replacements have been called “one of the best operations in medicine” and “the operation of the century”. I specialize in the direct anterior (front) approach to the hip which I first learned in 1987 during my residency training at Yale University.
Advantages of the Anterior Method Hip Replacement:
First Advantage of the Anterior Approach to the Hip:
Using the anterior hip replacement approach, there is a dramatic reduction in hip dislocations compared to the posterior hip approach which allows me to eliminate ALL hip precautions immediately after surgery. This means my patients are allowed to squat, tie their shoes, twist, cross their legs and do whatever they want immediately after their hip replacement. This is a huge advantage for the anterior approach compared to the posterior approach to the hip.
I have seen many patients' stress melt away after anterior surgery when they realize they don't need to worry about their hip replacement dislocating.
Most patients in the United States undergo a posterior approach total hip replacement which usually requires many weeks of strict precautions so the total hip does not dislocate. These precautions include no bending the hip past 90 degrees, no reaching down low, no crossing legs, and no sitting on a low toilet seat.
These hip restrictions after posterior surgery can be stressful for many patients due to the fear and real risk of a dislocating total hip.
What is a hip dislocation and why is it important to avoid?
When the ball of the hip (femoral head) pops out of the hip socket (acetabulum), a dislocation occurs which is about the most painful thing you could ever experience. A dislocated total hip at home means you call "911" for an ambulance to go back to the hospital for a "closed reduction" under anesthesia in the emergency room or operating room. Sometimes more open hip surgery is required.
After the closed hip reduction, you are required to wear a big hip brace 24 hours a day for 6-12 weeks. You should not remove the hip brace to shower.
The obvious conclusion here is: don't dislocate your total hip!
The anterior hip replacement approach helps maximize hip stability and avoid hip dislocation, especially compared to the posterior hip approach.
Second Advantage of the Anterior Approach to the Hip:
A second advantage unique to the anterior approach to the hip is that no muscle or tendon is cut or repaired later. The approach is "muscle splitting" and "muscle sparing" where muscles are simply spread sideways. At the end of surgery the muscles just fall back together. Other approaches to the hip require that tendons and muscle are cut off of bone then stitched back to bone. No tendons or muscle are stitched back with the anterior hip approach. I have performed all the approaches to the hip over the years. My personal experience is that my anterior hip patients hurt less and recover quicker because of this muscle splitting and muscle sparing approach.
Third Advantage of the Anterior Approach to the Hip:
A third advantage unique only to the anterior hip approach is the use of fluoroscopy or X-ray pictures during surgery to visualize BOTH hips. This X-ray technique helps with the precise, efficient placement of hip implants.
Fourth Advantage of the Anterior Approach to the Hip:
I use a special hip operating table (Hana table) designed specifically for anterior hip replacements which makes surgery much easier and more efficient.
My goal after an anterior approach total hip replacement is to eliminate fear in my patients and create confidence that they will have a pain free, strong hip replacement that will last for decades.
Hip Joint
The hip joint is the largest weight-bearing joint in the human body. It is also referred to as a ball and socket joint and is surrounded by muscles, ligaments, and tendons. The thigh bone or femur and the pelvis join to form the hip joint.
Any injury or disease of the hip will adversely affect the joint's range of motion and ability to bear weight.
The hip joint is made up of the following:
- Bones and joints
- Ligaments of the joint capsule
- Muscles and tendons
- Nerves and blood vessels that supply the bones and muscles of the hip
Bones and Joints
The hip joint is the junction where the hip joins the leg to the trunk of the body. It is comprised of two bones: the thigh bone or femur and the pelvis which is made up of three bones called ilium, ischium, and pubis. The ball of the hip joint is made by the femoral head while the socket is formed by the acetabulum. The Acetabulum is a deep, circular socket formed on the outer edge of the pelvis by the union of three bones: ilium, ischium, and pubis. The lower part of the ilium is attached by the pubis while the ischium is considerably behind the pubis. The stability of the hip is provided by the joint capsule or acetabulum and the muscles and ligaments which surround and support the hip joint.
The head of the femur rotates and glides within the acetabulum. A fibrocartilagenous lining called the labrum is attached to the acetabulum and further increases the depth of the socket.
The femur or thigh bone is one of the longest bones in the human body. The upper part of the thigh bone consists of the femoral head, femoral neck, and greater and lesser trochanters. The head of the femur joins the pelvis (acetabulum) to form the hip joint. Next, to the femoral neck, there are two protrusions known as greater and lesser trochanters which serve as sites of muscle attachment.
Articular cartilage is the thin, tough, flexible, and slippery surface lubricated by synovial fluid that covers the weight-bearing bones of the body. It enables smooth movements of the bones and reduces friction.
Ligaments
Ligaments are fibrous structures that connect bones to other bones. The hip joint is encircled with ligaments to provide stability to the hip by forming a dense and fibrous structure around the joint capsule. The ligaments adjoining the hip joint include:
- Iliofemoral ligament: This is a Y-shaped ligament that connects the pelvis to the femoral head at the front of the joint. It helps in limiting the over-extension of the hip.
- Pubofemoral ligament: This is a triangular shaped ligament that extends between the upper portion of the pubis and the iliofemoral ligament. It attaches the pubis to the femoral head.
- Ischiofemoral ligament: This is a group of strong fibers that arise from the ischium behind the acetabulum and merge with the fibers of the joint capsule.
- Ligamentum teres: This is a small ligament that extends from the tip of the femoral head to the acetabulum. Although it has no role in hip movement, it does have a small artery within that supplies blood to a part of the femoral head.
- Acetabular labrum: The labrum is a fibrous cartilage ring which lines the acetabular socket. It deepens the cavity, increasing the stability and strength of the hip joint.
Muscles and Tendons
A long tendon called the iliotibial band runs along the femur from the hip to the knee and serves as an attachment site for several hip muscles including the following:
- Gluteals: These are the muscles that form the buttocks. There are three muscles (gluteus minimus, gluteus maximus, and gluteus medius) that attach to the back of the pelvis and insert into the greater trochanter of the femur.
- Adductors: These muscles are located in the thigh which helps in adduction, the action of pulling the leg back towards the midline.
- Iliopsoas: This muscle is located in front of the hip joint and provides flexion. It is a deep muscle that originates from the lower back and pelvis and extends up to the inside surface of the upper part of the femur.
- Rectus femoris: This is the largest band of muscles located in front of the thigh. They also are hip flexors.
- Hamstring muscles: These begin at the bottom of the pelvis and run down the back of the thigh. Because they cross the back of the hip joint, they help in extension of the hip by pulling it backward.
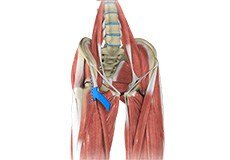
Nerves and Arteries
Nerves of the hip transfer signals from the brain to the muscles to aid in hip movement. They also carry the sensory signals such as touch, pain, and temperature back to the brain.
- The main nerves in the hip region include the femoral nerve in the front of the femur and the sciatic nerve at the back. The hip is also supplied by a smaller nerve known as the obturator nerve.
- In addition to these nerves, there are blood vessels that supply blood to the lower limbs. The femoral artery, one of the largest arteries in the body, arises deep in the pelvis and can be felt in front of the upper thigh.
Hip Movements
All of the anatomical parts of the hip work together to enable various hip movements. Hip movements include flexion, extension, abduction, adduction, circumduction, and hip rotation.

Hip Arthritis
Osteoarthritis, also called degenerative joint disease, is the most common form of arthritis. It occurs most often in the elderly. This disease affects the tissue covering the ends of bones in a joint called cartilage.

Hip Fractures
Pelvic fracture is a condition that arises due to breakage of the pelvis bones. It may damage internal organs, nerves, and blood vessels associated with the pelvis region.

Hip Bursitis
Hip bursitis is a painful condition caused by the inflammation of a bursa in the hip. Bursae are fluid-filled sacs present in the joints between bone and soft tissue to reduce friction and provide cushioning during movement.

Hip Dislocation
The hip joint is a “ball and socket” joint. The “ball” is the head of the femur or thighbone, and the “socket” is the cup-shaped acetabulum.

Snapping Hip
Snapping hip syndrome is a condition in which you hear or feel a snapping sound in the hip when you swing your legs, run, walk or get up from a chair. The sound can be experienced in the back, front or side of the hip.
Anterior Hip Replacement
Anterior Hip Replacement is a minimally invasive, muscle sparing surgery using an alternative approach to traditional hip replacement surgery.

Total Hip Replacement
Hip replacement has become necessary for your arthritic hip: this is one of the most effective operations known and should give you many years of freedom from pain.




